
Ascites and Paracentesis - Paracentesis
Paracentesis
2. "Ideal" Site
So far, we have been mainly discussing the techniques to detect peritoneal fluid and interpret its composition. The image acquisition and focus for the purposes of a paracentesis are a bit different.
1. Sonographic Landmarking
2. "Ideal" Site
1. Landmarking
You can place the probe always anywhere and perform the tap so long as there is NO critical structures nearby.
Usually, the right and left lower quadrants and flanks are the sites assessed.
The suprapubic area is usually avoided to presence of the bladder; and the least dependent region of the abdomen (depending on the patient's position) is, also, usually less favoured as the small bowel tends to float towards it.
You can place the probe always anywhere and perform the tap so long as there is NO critical structures nearby.
Usually, the right and left lower quadrants and flanks are the sites assessed.
The suprapubic area is usually avoided to presence of the bladder; and the least dependent region of the abdomen (depending on the patient's position) is, also, usually less favoured as the small bowel tends to float towards it.

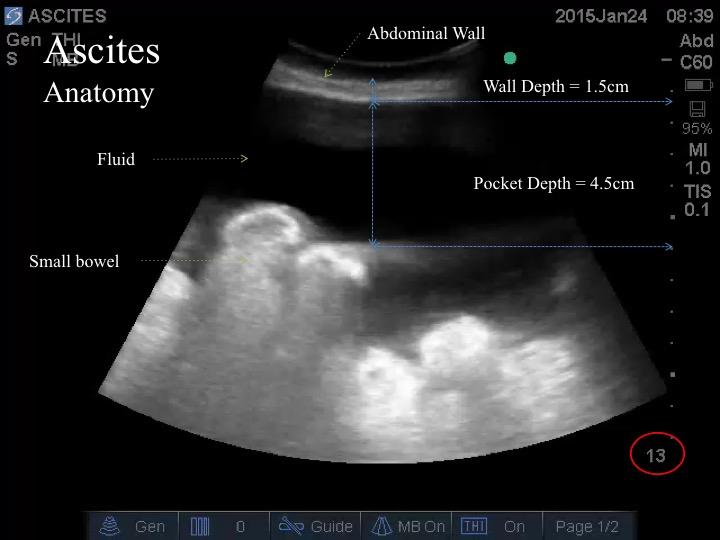
2. "Ideal" Paracentesis Site:
- No adjacent critical structure
- Needle will not reach critical structure accounting for dynamic changes
- Most dependent aspect of the pocket
- Shortest entry distance into the thoracic cavity
In this plane, there is a pocket with no viscera in the path. However, when the probe is translated slightly, a small piece of viscera appears.
The needle is at risk of puncturing the viscera.
Always sweep to “clear” a site.
The needle is at risk of puncturing the viscera.
Always sweep to “clear” a site.
Linear probe yields high resolution of the abdominal wall for depth and vessels, ascites depth, and visceral organs just beneath.
Image is taken at the right flank at the mid-axillary line. In this case, the pocket depth is on 2cm deep - then the small bowel will be reached. This is a high risk spot.
Image is taken at the right flank at the mid-axillary line. In this case, the pocket depth is on 2cm deep - then the small bowel will be reached. This is a high risk spot.

Despite the small bowel is anchored to the mesentry, it does contain air, therefore it tends to float.
Image is taken from the top of a supine abdomen. The bowel is ~0.5cm away from the abdominal wall - extremely high risk of perforation if paracentesis is attempted.
Image is taken from the top of a supine abdomen. The bowel is ~0.5cm away from the abdominal wall - extremely high risk of perforation if paracentesis is attempted.

These images was taken from a spot at a bulging flank where a therapeutic paracentesis was attempted the day prior. In this image, the small bowel was adhered to the part of the peritoneum that was punctured.
The inflammation from the trauma may cause an adhesion.
Never assume that any spot is safe even if it was prior.
The inflammation from the trauma may cause an adhesion.
Never assume that any spot is safe even if it was prior.

Take Home Messages:
- Find the safest site to insert the needle
- Use a need with a length less the sum of the Wall Depth and Fluid Pocket Depth
- Beware of critical structures adhering to the peritoneal wall at the sites of trauma (eg. previous paracentesis)
- Scan anyone with an ascites
- Identify the diaphragm
- Identify the intra-abdominal structures
- Identify the “ideal” paracentesis spot