
Pneumothorax - Evidence
a. CXR vs PoCUS:
Is PoCUS any good at detecting pneumothorax compared to what has had been done in clinical practice for past several decades?
Well, that depends on what you are comparing it with. Currently, the Gold Standard diagnostic radiographic modality is CT scan of the thorax. However, in practice, CT scans are not obtained frequently to rule out a pneumothorax. CXR is the conventional diagnostic radiographic modality of choice due to (a) ease of access, (b) rapid turnover, and (c) relatively inexpensive compared to a CT thorax. However, despite CXR is high specific, it is notoriously insensitive. So how does PoCUS fair in comparison to CXR?
Meta-Analysis by Alrajab et al. in 2013 demonstrated that PoCUS is superior to CXR with CT thorax as the gold standard comparison.
Is PoCUS any good at detecting pneumothorax compared to what has had been done in clinical practice for past several decades?
Well, that depends on what you are comparing it with. Currently, the Gold Standard diagnostic radiographic modality is CT scan of the thorax. However, in practice, CT scans are not obtained frequently to rule out a pneumothorax. CXR is the conventional diagnostic radiographic modality of choice due to (a) ease of access, (b) rapid turnover, and (c) relatively inexpensive compared to a CT thorax. However, despite CXR is high specific, it is notoriously insensitive. So how does PoCUS fair in comparison to CXR?
Meta-Analysis by Alrajab et al. in 2013 demonstrated that PoCUS is superior to CXR with CT thorax as the gold standard comparison.
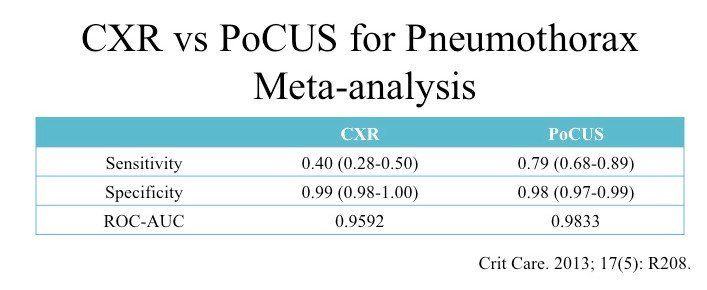
In terms of specificity, CXR is superior to PoCUS though only marginally. On a CXR, if you see a pneumothorax, it is usually quite obvious. However, it is less obvious with PoCUS. You need to evaluate multiple thoracic signs to determine whether the integrated permutation of sonographic signs corroborate with a pneumothorax.
Nevertheless, CXR is highly insensitive compared to PoCUS. This is not a major surprise. Pneumothorax can generally be seen provided it is an erect CXR, the pneumothorax is not loculated, and sizeable enough to be seen. However, in practice, most sick patients cannot stand or maintain an adequate erect position in bed. If the pneumothorax is too small, you cannot see it, or it is hidden behind the first rib.
The advantage of PoCUS is that it can be deployed in the supine and the individual signs have high operational characteristics on ruling out pneumothorax. The problem is that the probe can only see so much of the thorax at a time -- can only interrogate the region of the thorax scanned.
Nevertheless, CXR is highly insensitive compared to PoCUS. This is not a major surprise. Pneumothorax can generally be seen provided it is an erect CXR, the pneumothorax is not loculated, and sizeable enough to be seen. However, in practice, most sick patients cannot stand or maintain an adequate erect position in bed. If the pneumothorax is too small, you cannot see it, or it is hidden behind the first rib.
The advantage of PoCUS is that it can be deployed in the supine and the individual signs have high operational characteristics on ruling out pneumothorax. The problem is that the probe can only see so much of the thorax at a time -- can only interrogate the region of the thorax scanned.
b. Lung Sliding:
Of all the pneumothorax sonographic features that have been discussed, lung sliding has been most studied.
Of all the pneumothorax sonographic features that have been discussed, lung sliding has been most studied.

Multiple studies have consistently demonstrated the presence of lung sliding has higher sensitivity in comparison to CXR. With a sensitivity of 95-100%, clinically acceptable operational characteristic to rule out a pneumothorax.
c.
Lung Pulse:
The original study that described this sonographic phenomenon did not evaluate lung pulse in those with pneumothorax. 15 right main stem intubations were purposely performed in those WITHOUT pneumothorax.
The original study that described this sonographic phenomenon did not evaluate lung pulse in those with pneumothorax. 15 right main stem intubations were purposely performed in those WITHOUT pneumothorax.
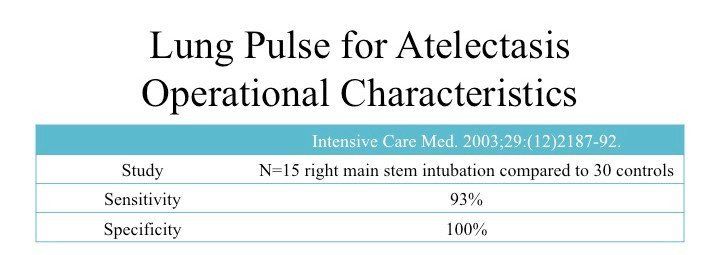
Given that the lung pulse can only be generated when the VPPI is apposed, a pneumothorax will obliterate this sign. Hence, the results of this study have had been EXTRAPOLATED and APPLIED to the lung pulse for pneumothorax. There has been no further studies to evaluate this sonographic sign in the context of a true pneumothorax.
This sign depends on the transmission of the cardiac impulse to the VPPI. One would reason the closer to the heart (Z1-2), the easier it is to the lung pulse; and the farther it is from the heart (Z4-6), the weaker lung pulse transmission.
This sign, however, is most useful in the context of no active respiration movement (between respiratory cycles, or apnea), or absence of air flow into the region of lung being evaluated (one lung ventilation, bronchial occlusion).
This sign depends on the transmission of the cardiac impulse to the VPPI. One would reason the closer to the heart (Z1-2), the easier it is to the lung pulse; and the farther it is from the heart (Z4-6), the weaker lung pulse transmission.
This sign, however, is most useful in the context of no active respiration movement (between respiratory cycles, or apnea), or absence of air flow into the region of lung being evaluated (one lung ventilation, bronchial occlusion).
d.
Lung Point:
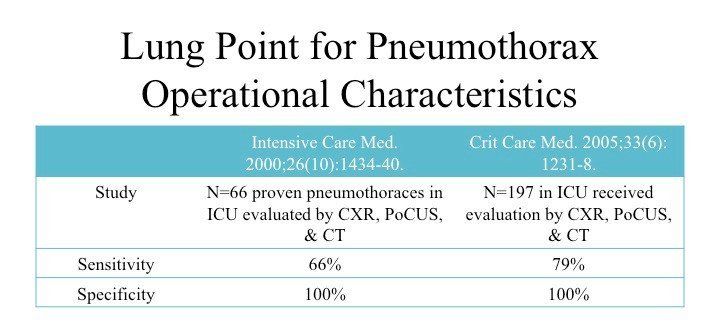
Only the following two studies by the same author have explicitly evaluated the operational characteristics of the Lung Point.
Only the following two studies by the same author have explicitly evaluated the operational characteristics of the Lung Point.
Given that by definition the sonographic lung point is where the
visceral pleura of the lung contacts the parietal pleura of the
pneumothorax during respiration, the lung point, not surprisingly, has a very high specificity. However, there are lung point mimics (cardiac to lung interface, diaphragm to lung interface) that can result in false positive interpretations yielding a lower specificity. In the above two studies, no such false positive lung point was reported.
With regards to sensitivity, the lung point performs rather poorly. The problem is finding the interface between the pneumothorax and where the lung parenchyma that still contacts the parietal pleura on the thorax. Also, massive pneumothorax that envelopes the entire lung parenchyma will not exhibit a lung point.
With regards to sensitivity, the lung point performs rather poorly. The problem is finding the interface between the pneumothorax and where the lung parenchyma that still contacts the parietal pleura on the thorax. Also, massive pneumothorax that envelopes the entire lung parenchyma will not exhibit a lung point.
Take Home Messages:
- PoCUS is more sensitive than CXR for pneumothorax
- Presence of lung sliding rules out pneumothorax
- Presence of lung point rules in pneumothorax