
IVC - Pitfalls
Pitfalls of the Inferior Vena Cava
1. Cylinder Effect
The IVC can be geometrically described as a cylinder. However, it is actually more of an oval cylinder than a perfect circle -- wider than its height.
When imaging a cylinder in the short or long axis, if the plane is not cut currently, the true diameter of the cylinder can be over or under-estimated.
Cylinder Effect in Long Axis Imaging
When the IVC is imaged on its long axis, if the probe is displaced just lateral to the center where the true diameter is located (Black), it will be underestimated (Red).
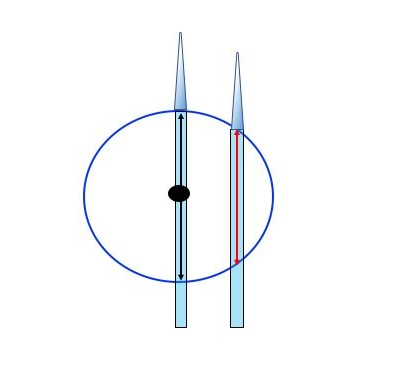
The way you troubleshoot the long axis cylinder effect problem is by sliding the probe side to side until you find the plane that yields the widest IVC diameter.
Cylinder Effect in Short Axis Imaging
When the IVC is imaged on it short axis, if the probe is tilted, a falsely overestimated diameter (Red) will be measured in comparison to the true diameter (Black) when the probe is perpendicular to the IVC.
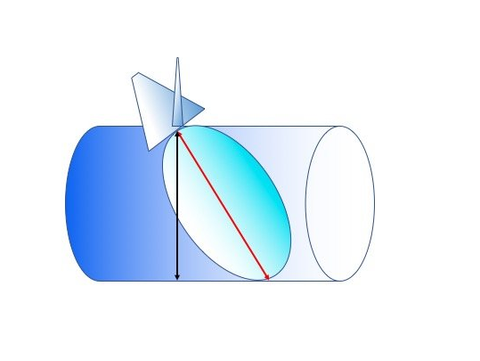
The way you troubleshoot the short axis cylinder effect problem is by tilting or fanning the probe until you find the plane that yields the shortest IVC diameter.
2. IVC Displacement during Respiration
When imaging the IVC, whether it be long or short axis, the probe is placed at
on the body (ie. you do not move the probe after you found a good imaging window), then one interprets the IVC's respiratory variation on the monitor by measuring the collapsibility at a reference cross section of the IVC (ie. with the aid of M-mode). We intuitively think this reference point is fixed
during the measurement (so were are comparing the cross section during the entire process), but, in fact, it is displaced during respiration.
The respiratory motion (eg. abdominal movement and internal organ displacements) will result in displacement of that reference point.
Cranio-caudal Displacement
This will be the error introduced when the IVC is imaged in the short axis.
Medial-lateral Displacement
This will be the error introduced when the IVC is imaged in the long axis.
A study by Blehar et al (Blehar et al. Critical Ultrasound Journal 2012, 4:18) found that the average displacements were:
- Cranio-caudal displacement: 2.17cm (95% CI 1.8 to 2.5cm)
- Medial-lateral displacement: 0.39cm (95% CI 0.33 to 0.45cm)
These displacements can affect how we measure collapsibility via M-mode or "eye-balling". It is, therefore, important to survey the IVC in general rather than just a one point.
3. Respiratory Effort
The inspiratory effort induced by a spontaneously
breathing patient greatly affects the collapsibility of the IVC. It has been demonstrated that the greater diaphragmatic excursion the greater IVC collapsibility. (Anesthesiology 2016; 124:1338-46)
There is no studied and tested method of inspiration for IVC collapsibility for a spontaneous
breathing patient, thus. The "Sniff" maneuver is utilized by during echocardiography as a standardization.
However, in practice, the acutely ill will exhibit varying degrees of respiratory effort. Not only that, the correlation between respiratory effort and diaphragmatic excursion is not straightfoward. The complex interplay between the chest wall, lungs, and abdomen affect this relationship.
This confounder is difficult to deal with, but, like anything else in medicine, always
interpret the IVC along with the clinical context. Do not interpret the IVC in isolation: fit the data to the clinical picture, not vice versa.
For example, when you see an IVC collapsing significantly, take note of the patient's respiratory effort. If the patient is using accessory muscles, interpretation would be difficult. However, if the IVC is not collapsing despite significant respiratory effort, the central venous pressure is likely very high.
4. What does the IVC clinically mean?
As eluded on the Mythbusting section, the clinical meaning of IVC collapsibility is NOT that dichotomous.
Take Home Points
- IVC is not so simple
- Must interpret the IVC in the clinical context: use every data point you have to make sense of the collapsibility you see