
Pneumothorax - Knobology and Probe Selection
Knobology and Imaging Technique
2. Knobology Optimization
3. Image Acquisition
Parenchyma PoCUS has its specific Image Acquisition finesses that are crucial to producing high quality images:
1. Probe Selection
2. Knobology Optimization
3. Image Acquisition
1. Probe Selection:
Linear: The probe of choice given its high frequency bandwidth to resolve the pleural line (VPPI) - the focus of this PoCUS indication.
Curvilinear: If you have no access to the Linear probe, the curvilinear probe may suffice IF you can visualize the pleural line.
Phased-Array: Pleural line imaging with this probe is very poor - do not use this.
Linear: The probe of choice given its high frequency bandwidth to resolve the pleural line (VPPI) - the focus of this PoCUS indication.
Curvilinear: If you have no access to the Linear probe, the curvilinear probe may suffice IF you can visualize the pleural line.
Phased-Array: Pleural line imaging with this probe is very poor - do not use this.

2. Knobology - Optimal Settings:
- Depth: Adjust the Depth so the visual real estate of the pleura is maximized
- Focal Zone: Focus it at the Pleural Line
- THI:Turn Off - to improve artifact generation for A-Lines and Vertical Lines
3. Image Acquisition - Where to scan?
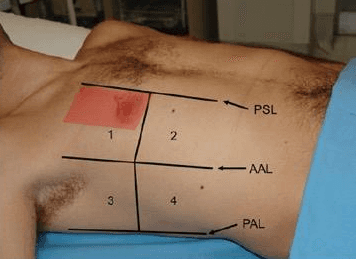
- Position the patient in supine position – flat.
- Place the probe at the least dependent region: ~2-4ICS bounded by the clavicle, PSL, and MCL = region shaded red Position the probe perpendicular to the ICS with the indicator pointing cranially (preferred).
- If an area along the above peristernal space exhibits signs suggestive of a pneumothorax, then slide the probe laterally to look for the pneumothorax-parenchymal boundary (seen below)
Key:
Maintain the probe perpendicular to the pleura
(≠ to perpendicular to the chest wall) for the highest resolution and lung ultrasound artifacts.
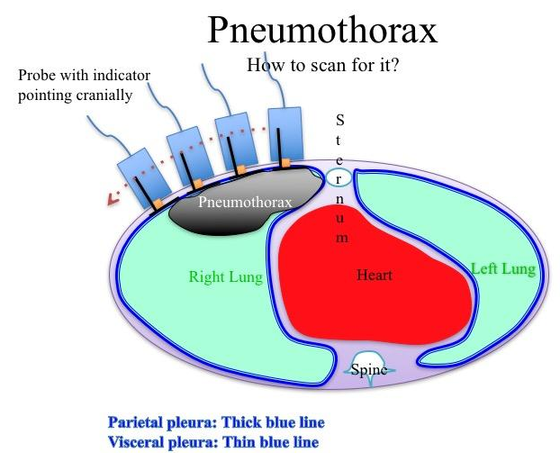
Here is a schematic diagram of pneumothorax imaging.
The pneumothorax floats up to the most independent region of the thorax. The probe, which is placed at this region at the peristernal area, detects signs suggestive of a pneumothorax. Then slide the probe laterally to look for the parenchyma and pneumothorax boundary/interface (Lung Point).
The pneumothorax floats up to the most independent region of the thorax. The probe, which is placed at this region at the peristernal area, detects signs suggestive of a pneumothorax. Then slide the probe laterally to look for the parenchyma and pneumothorax boundary/interface (Lung Point).
The above technique assumes the following:
(a) the pneumothorax is not loculated -- so the air will float to the most independent region in the thorax
(b) the air will float to the most independent region in the thorax
With regards to the former, PoCUS will have poor sensitivity if it is not locuated in the most independent region. However, loculated pneumothorax are not clinically dangerous.
The latter, however, has major implication to the sensitivity of PoCUS for pneumothorax. Where is the most independent region? It all depends on the patient's position and thoracic morphology. Although most texts describes scanning the 2-4th ICS peristernal region in the supine patient, some studies have shown that a significant portion of pneumothoraces accumulate in the lower thorax - 5-8th ICS. (Am J Emerg Med. 2012;30:(7)1025-31. Crit Care Med. 2005;33:(6)1231-8.)
It is quite quick and easy to rapidly scan along the entire peristernal region to improve sensitivity.
Take Home Messages:
- Use the Linear Probe for pneumothorax evaluation
- Place the patient in supine and image the most dependent region of the throax - two presumptions for the described technique:
- Air will float up to this region: the pneumothorax is not loculated
- The pocket of air will float to the region being scanned - can miss it if the air did not collect there, or if it is shielded behind bone