
Lung Parenchyma - Lung Parenchyma
Lung Parenchyma
1. Language and Definition Standardization
2. Individual Signs
a. A-Lines
b. B-Lines
c. Hepatization
d. Fractal Sign (aka. Shred Sign)
e. Air Bronchogram
1. Language and Definition Standardization
2. Individual Signs
a. A-Lines
b. B-Lines
c. Hepatization
d. Fractal Sign (aka. Shred Sign)
e. Air Bronchogram
1. Language and Definition Standardization
In 2012, an International consensus was published to standardized the terminologies, definition, and criteria for Thoracic PoCUS.
This is particularly important for parenchymal PoCUS as its utility is founded on artifact interpretation.
If you read the older literature, you will find various terminologies used to describe the same entities - can be quite confusing.
Do read this document.
In 2012, an International consensus was published to standardized the terminologies, definition, and criteria for Thoracic PoCUS.
This is particularly important for parenchymal PoCUS as its utility is founded on artifact interpretation.
If you read the older literature, you will find various terminologies used to describe the same entities - can be quite confusing.
Do read this document.

Consensus Statement Excerpts are as follows (ICM. 2012;38:577-591.):
“B-lines are defined as discrete laser-like vertical hyperecholic reverberation artifacts that arise from the pleural line (previously described as “comet tails”), extend to the bottom of the screen without fading, and move synchronously with lung sliding.” (Level N/A)
“A positive region is defined by the presence of three or more B-lines in a longitudinal plane between two ribs.” (Level A)
“B-lines are defined as discrete laser-like vertical hyperecholic reverberation artifacts that arise from the pleural line (previously described as “comet tails”), extend to the bottom of the screen without fading, and move synchronously with lung sliding.” (Level N/A)
“A positive region is defined by the presence of three or more B-lines in a longitudinal plane between two ribs.” (Level A)
2. Individual Signs
a. A-Lines
Criteria:
a. A-Lines
Criteria:
- Curved arcs inferior to the pleural line
- Mirror images of the pleural line
- Distance between the Pleura and 1st A line = to the distance between all other subsequent A lines
- Theorectially, A-lines will continue to appear regardless of depth though in reality they eventually are attenuated
- A-lines = Air in Thorax (pleural space, or normal parenchyma)

Apply the criteria described above - see if they fit the findings in this scan.
In this scan, you can see two A-Lines deep to the pleural line. This indicates that there is air in the THORAX (pleural space or parenchyma). Given that pleural sliding is present, the VPPI is apposed, therefore there is no pneumothorax.
In this scan, you can see two A-Lines deep to the pleural line. This indicates that there is air in the THORAX (pleural space or parenchyma). Given that pleural sliding is present, the VPPI is apposed, therefore there is no pneumothorax.
b. B-Lines
Criteria:
Criteria:
- Originates at the pleural line – not superior or inferior to it
- Narrow beam profile proximal, then widens in caliber distally
- Vertical lines that reach the bottom of the screen
- Moves with respiration
- >3 B lines in a scanned zone is considered as “Significant”
- B-lines = Interstitial syndrome

Apply the criteria described above - see if they fit the findings in this scan.
In this scan, you can see many vertical lines originating from the VPPI. In fact, there are so many that it is difficult to distinguish the individual lines -- so called "Search Light" Sign.
In this scan, you can see many vertical lines originating from the VPPI. In fact, there are so many that it is difficult to distinguish the individual lines -- so called "Search Light" Sign.
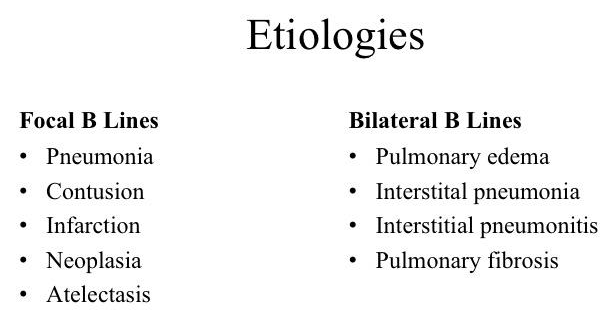
Interstitial Syndrome:
something that is not normally present is occupying the interstitial space.
What can they be? Blood, Pus, Water, Cell, Fibrosis
Based on the B-Line distribution pattern and other syndrome specific sonographic features, one can narrow the differential diagnosis with PoCUS alone.
What can they be? Blood, Pus, Water, Cell, Fibrosis
Based on the B-Line distribution pattern and other syndrome specific sonographic features, one can narrow the differential diagnosis with PoCUS alone.
c. Hepatization
Criteria:
Criteria:
- Parenchyma exhibits solid organ (eg. liver) like echogenic features
- Consolidation - lung
- Mass

Clip i.
Hepatization due to left main bronchus compression from a mediastinal mass
Clip ii.
Hepatization due to mass infiltration of the lung parenchyma (ie. sarcocarcinoma)
Clip iii.
Hepatization due compression from pleural effusion
d. Fractal Line: Border/interface between consolidated and aerated lung
Features:
Features:
- Irregular, coarse, discontinued line
- May move with respiration
- B-lines may arise from the line
- Pleural line cannot be seen
- Hypoechoic/Anechoic signal above the line is the consolidated lung
- Effusion (anechoic signal) can be distinguished from a consolidation via the presence of a smooth lung line borders the former and a shredded line borders the latter
- Consolidation - lung
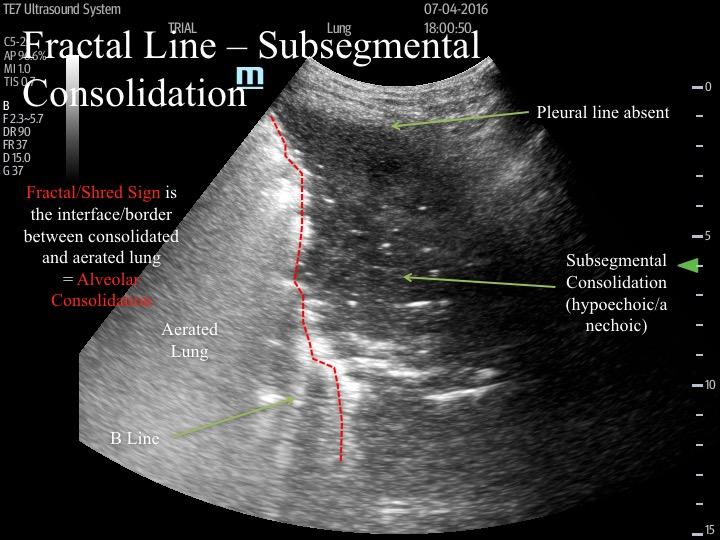
This particular sign is not as easy to grasp since the sonographic features are bit less concrete. We will use a schematic diagram to explain what you are looking at.
Suppose the stone tiles is the aerated alveolar air space and the cracks in between are the interlobular septae - parenchyma.
If a region is filled completely by something, let's say Pus, it will be consolidated. The border between the consolidated (non-aerated lung) and the aerated lung is the fractal line - as demarcated in red.
Suppose the stone tiles is the aerated alveolar air space and the cracks in between are the interlobular septae - parenchyma.
If a region is filled completely by something, let's say Pus, it will be consolidated. The border between the consolidated (non-aerated lung) and the aerated lung is the fractal line - as demarcated in red.

e. Air Bronchogram:
anatomically, it reflects air-filled airway surrounded by air devoid alveoli (consolidation)
Features:
Features:
- Linear vs Punctiform
- Dynamic vs Adynamic
Clip i. Air Bronchograms:
Two manifestations are shown here - Linear (line shaped) and Dynamic (moving with respiration)
Clip ii. Air Bronchograms:
Two manifestations are shown here - Punctate (dot shaped) and Adynamic (not moving with respiration)
Clip iiia. No Air Bronchograms -
complete atelectasis of the RLL due to complete occlusion of the bronchus resulting in absorption atelectasis. Note that you can see some anechoic tubes running in the parenchyma. Are they airways or vessels?
Clip iiib. Air Bronchogram versus Vasculature - Putting Colour Doppler on the tubes revealed evidence of flow - some are even pulsatile. hence, they are vessels.
Take Home Messages:
- Parenchyma sonographic findings primarily consist of artifacts generated at the VPPI
- Abnormal parenchymal sonographic findings can ONLY be detected if the VPPI is involved (if the abnormality was proximal with no peripheral involvement, US will not be able to detect the problem)
- A-Lines = Air in the Thorax
- in conjunction with the presence of pleural sliding = normal thorax
- B-Lines = Interstitial Syndrome
- wide differential, but can narrow based on distribution patterns and associated findings
- Hepatization = Consolidation
- Fractal Line = Subsegmental Consolidation - border between consolidation and aerated lung
- Air Bronchograms = Feature of consolidation