
Pericardial Effusion - Image Interpretation
1. Anatomy
The following images illustrate how a large pericardial effusion appears on each of the standard windows of the heart.
However, the take home point here is to note whether the effusion accumulation is Circumferential
(ALL around) vs Regional (just accumulating at one spot).
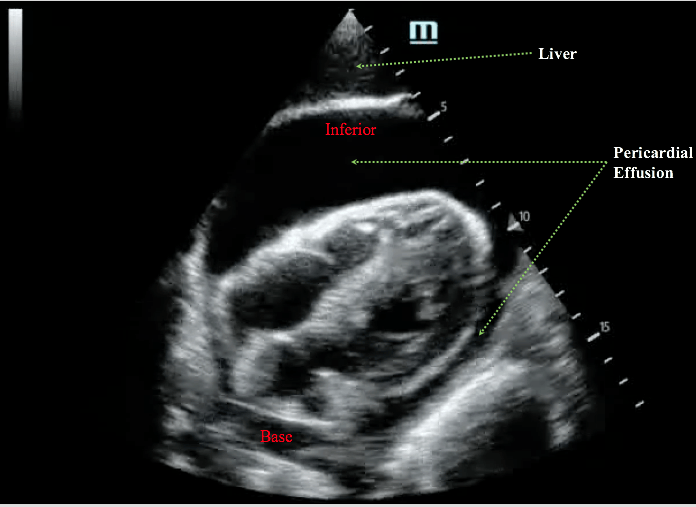
a. Subcostal View
It is quite easy to view the entire circumferential space from this view. Recall that subcostal view images the heart from the inferior aspect.
Pericardial fluid tend to accumulate in this region adjacent to the free wall of the right atrium and right ventricle due to gravity.
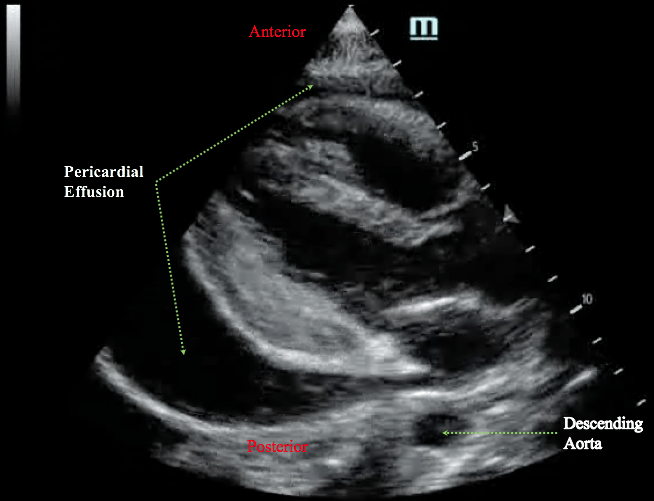
2. Parasternal Long View
The key landmark relevant to the pericardial effusion imaging from this view is the descending aorta. Anterior to the descending aorta is the pericardial sac, and posterior to it is the left pleural space.
Hence, the pericardial effusion tracks ANTERIOR to the descending aorta, and pleural effusion tracks POSTERIOR to the descending aorta.
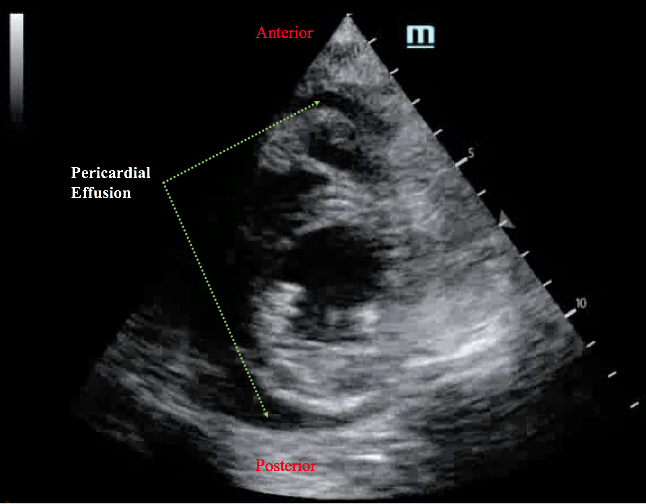
3. Parasternal Short View
This view will demonstrate accumulation of the pericardial fluid anteriorly and posteriorly.
4. Apical 4 View
This view is not easy to obtain, so this should not be the first cardiac window of choice to image a pericardial effusion. However, this view is required to interrogate trans-valvular (tricuspid and mitral) flow profile to detect tamponade physiology.

2. Pericardial Effusion Appearance
There are two basic appearance of pericardial effusion:
- Simple: anechoic appearance with nothing inside it
- Complicated: echoic things are in the fluid
3. Effusion Size
The size of the pericardial effusion sonographically characterized by the diameter of the deepest pocket during diastole:
- Small: <1cm
- Medium:
1-2cm
- Large: >2cm
The KEY point is that effusion size does not correlate with hemodynamic instability. A hyperacutely accumulated yet small pericardial effusion can result in tamponade. However, a chronically accumulated yet large pericardial effusion may well be hemodynamically stable.
Nevertheless, medium and especially large pericardial effusion may decompensate hemodynamically due to further accumulation resulting in tamponade, or via other hemodynamic stressors (eg. hypovolemia).
Take Home Messages:
- When describing the pericardial effusion:
- Circumferential vs Regional
- Simple vs Complicated
- Small, Medium, or Large